- Get started here
- Learn health science for yourself
- Create a health data spreadsheet
- Read your data with standard formats
- Symptoms
- Coming soon
- Example stories
- Coming soon
Learn health science for yourself
staty is focused on reading health data from a spreadsheet…
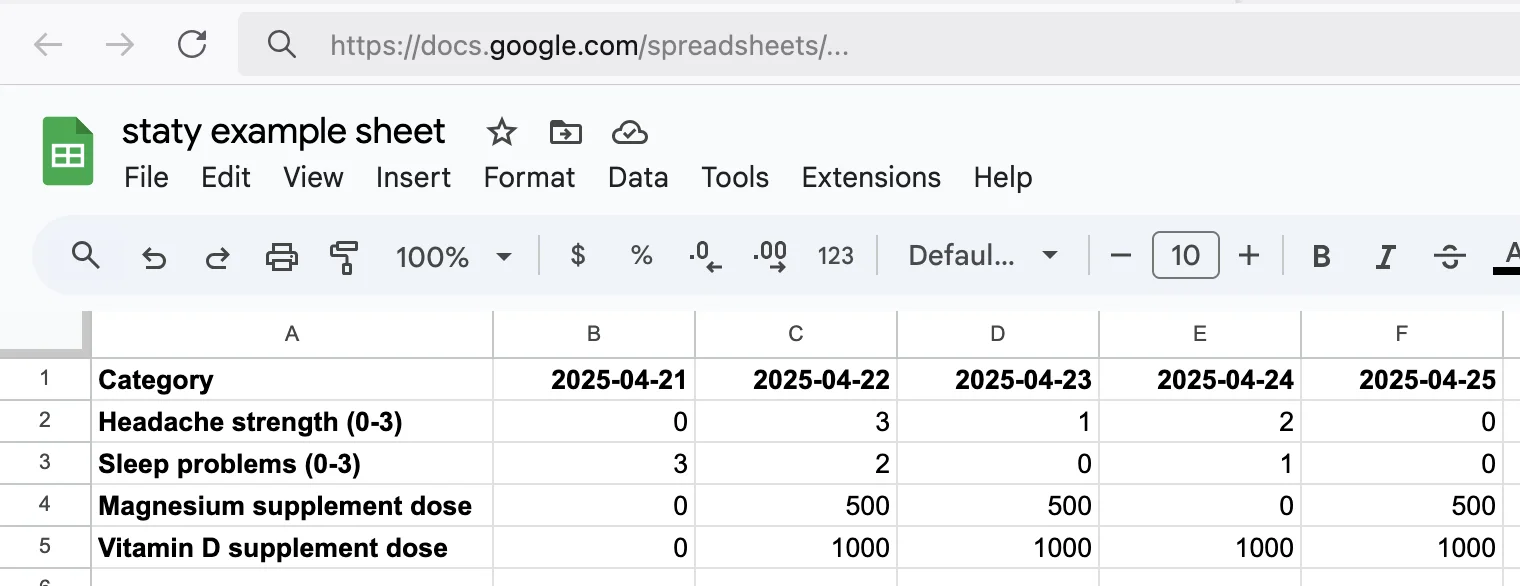
…to answer questions by analyzing the data:
That's science: note down observations, try interventions, use the data to compare what is better, remember and increase that knowledge.
But how does one know what to write down, which interventions to try, whether something works, and how to prove it?
Science for one individual person, also called "N=1 science", comes into play here. That person is you. In this guide, you'll learn the following:
- How science works: which types of studies exist, proving correlation and causation, a very tiny bit about statistics, benefits of N=1 science
- Interventions: decide which supplementation, medication, home remedy, exercises or other treatments to try depending on symptoms
- Why nobody else can care as much about your health as yourself, and why it's worth investing self-research effort
- Which self-observations, symptoms and other health data make sense to track, and which are useless
- How exactly to write down these observations
- How to keep your own research simple so that you'll actually keep doing it longterm, for your own benefit
- Where to find trusted scientific information and possibly helpful anecdotes online
- What your findings mean for yourself and other people, and how to share them (if desired)
Understand what you want to achieve
If you came here, you probably have health issues that you want to solve. Or maybe you want to find if there's something that could improve your sleep or well-being, without having strong symptoms. The goal must be to improve one or more outcomes: for example sleep quality, headache strength and frequency, mental illness or behavior, dizziness, brain fog, motivation, or whatever else you can think of. Outcomes must be measurable, and it's fine if you can only judge subjectively, such as on a scale from 0 to 10.
You do have one or more symptoms or outcomes that you want to improve? Good, now you have a clear goal and can get going without losing motivation.
Research stuff yourself
Reading, listening, understanding, exploring further… These are the basics for your own research of health topics. They are actually required to understand any topic better, and health and the human body are large, complicated topics.
This article teaches which information sources to use and trust, how not to take early or wrong conclusions, distinguish types of studies and data, and so on. The choice to start researching needs to come from yourself, and it's a choice anyone can make. The desire to understand your own health is the first step. Anyone willing to learn, observe, and think critically can become an informed advocate for their wellbeing.
Informing yourself is a new paradigm. Our previous generations could mostly only rely on doctors or newspaper articles. There simply were no other sources. Those sources largely defined their world view. We don't think that's nearly enough nowadays. Great news: the public internet offers free, very helpful sources and tools, and it's no longer the case that knowledge about health is restricted.
Here are some very simple steps to level up how you deal with health and science: bookmark PubMed and use it in addition to internet search engines like Google, follow well-known science journalists on social media for topics that interest you, question and double-check everything you read, get informed before and after your next doctor appointments (for example, become knowledgeable about your blood work values and their meaning). If you can do these, you're on a very good track.
In the long term, you need to have the diligence to search the internet and explain topics to yourself, even while reading this article. With that understanding, you'll also gain the courage to fix or totally reverse any old understanding of how health "works". We will later look at examples like the "saturated fat and cholesterol are bad" hypothesis that originated in the 1950's. It is still believed by so many people, despite all the corrective information being out there. In today's reality, new or fixed information can still take decades to circulate, despite us having the internet as great and free information source.
Large-scale science vs. single-person science
We tried to depict sizes of medical studies here. The "N" normally stands for the number of subjects, like humans or mice in an experiment group. Let's go through the different sizes since it's important to have a rough understanding how much trust can be put into which studies, and which results they can have in theory:

Or in other words:
- What can't big studies show? Individual benefits.
- What can't doctors do? Invest lots of time.
- What can a single person not find out alone? Whether a solution is the root cause, or works safely for everyone.
By combining the advantages of the study types, however, these downsides vanish. Below, we look at their properties.
Large-scale studies (N=large)
These studies come in different types:
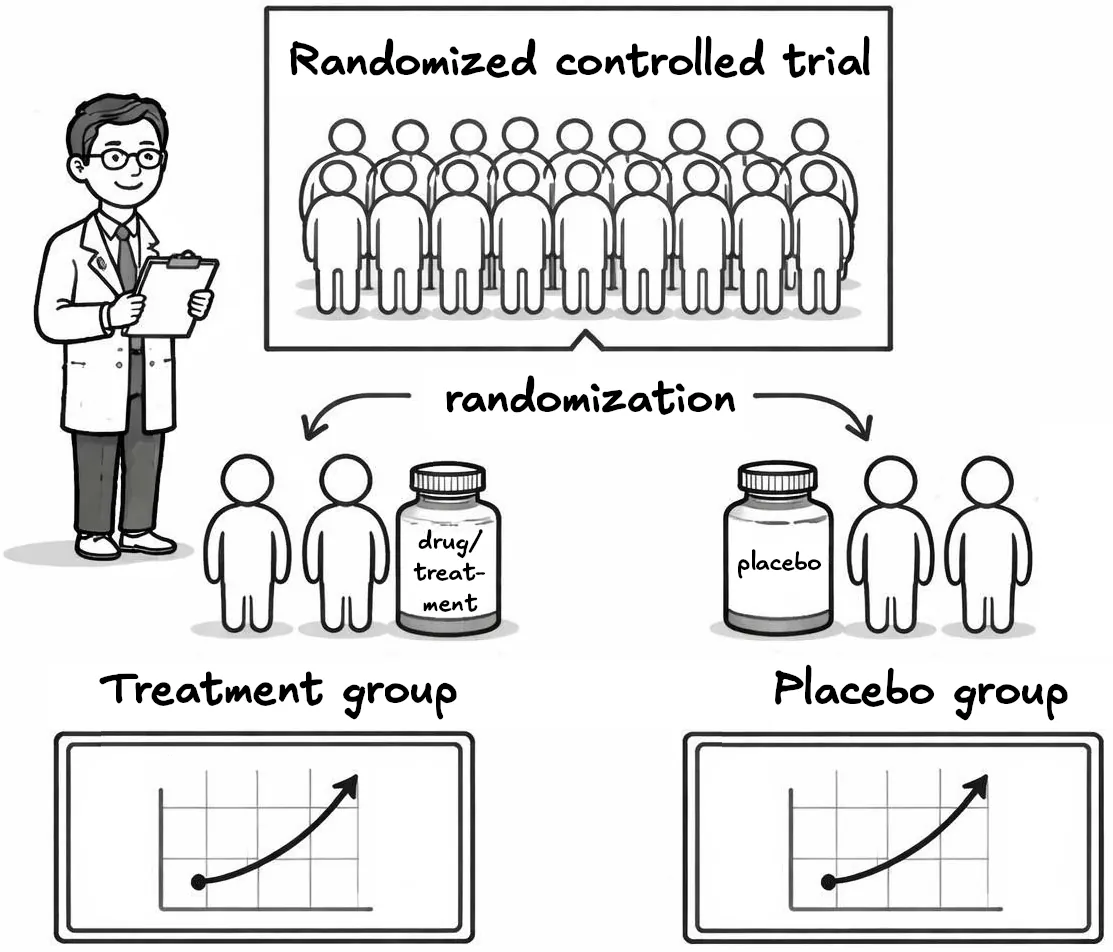
Participants are randomly assigned to different groups (e.g., treatment vs. placebo). This minimizes bias and is considered the gold standard for determining cause-and-effect relationships. At best, a study is double-blinded – both participants and researchers don't know who receives which treatment. It's costly and requires careful design, so it isn't used often.
A crossover design is sometimes used in addition: if there's one intervention and one control (e.g., a placebo), all participants receive both in random order, often with a "washout" period in between. This avoids inter-person variability since treatments are comparable for each person. Fewer participants are needed since each person serves as their own control.
Follows a group of people (cohort) over time, comparing outcomes between those exposed and not exposed to a particular factor. Useful for studying risk factors and disease progression.
Compares individuals with a disease (cases) to those without (controls), looking back to identify potential causes or risk factors. These are similar to cohort studies, but try to actively search for risk factors (and thereby possible causes) rather than retrospectively checking predefined, potential risk factors.
Observes a population at a single point in time, measuring the prevalence of outcomes and exposures. Cannot establish causality but useful for generating hypotheses – for example, to measure how common a disease or risk factor is.
Observes the same individuals repeatedly over time, tracking changes and relationships between variables. Useful for understanding development and long-term effects.
Brings together results from multiple studies on a specific question through exhaustive literature search and quality assessment. While RCTs are the gold standard for single studies, systematic reviews are best for summarized information on one topic.
Sometimes, a meta analysis is included: if treatment effects are comparable across found literature, they're compared to see whether a majority of studies support "intervention works" or "intervention doesn't work / does harm". This clarifies whether evidence is clear, or has mixed results.
Example: After Dinner Rest a While, After Supper Walk a Mile? [...] Acute Postprandial Glycemic Response to Exercise Before and After Meal Ingestion in Healthy Subjects and Patients with Impaired Glucose Tolerance: Searched for studies in type-2 diabetes patients which compared exercise before vs. after a meal, looking at blood glucose after the meal as an outcome.
In this example, a problem with the typical meta analysis charts is that here, both pre-meal and post-meal exercise could have an effect, as shown in real self-experiments, so plotting a graph with "favors pre-meal exercise" and "favors post-meal exercise" on the same axis probably doesn't easily visualize this fact. Experiments on yourself can largely vary from recommendations in large-scale study results!
Tests the safety and efficacy of new treatments in humans, often in phases. Can be randomized or non-randomized.
Describes a small group of patients with a similar condition or exposure, often used to report new or unusual findings. No control group, and therefore causality cannot be assessed.
More types and subtypes exist, but the above are the important ones.
The problem with most study types is that correlation doesn't prove causation. See spurious correlations (funny, but important!). Double-blinded RCTs can help prove causation, but aren't always possible, for example when it would be unethical (exposing one group to a known risk factor), hard to blind (placebo must match look and taste; exercise can't be replaced by placebo), have too few participants (rare diseases), or cost too much (multi-year follow-ups).
Also, the quality of inputs and observations may be poor. Many cohort studies rely on questionnaire data. NHANES (National Health and Nutrition Examination Survey), for example, surveys 5,000 people annually in the USA with questions about food habits. Could you accurately remember what and how often you ate certain foods? Should "red and processed meat" even be a single category – does a raw steak count the same as breaded meat with condiments and preservatives? Such problems make results highly inaccurate.
Example: Severe Headache or Migraine History Is Inversely Correlated With Dietary Sodium Intake: NHANES 1999–2004 used food questionnaire data to find that headache symptoms are less common with higher sodium intake (e.g., from table salt). But this can't simply justify recommending more salt since it could be dangerous towards other health outcomes.
No study type gives definite answers unless results are very strong. Cigarette smoking causing lung cancer is a rare example. But it still took many studies to prove the causal link. Looking at Smoking and Carcinoma of the Lung, a 1950 large-scale study, you might think in hindsight the numbers were totally obvious. But that's easy to say decades later, ignoring tobacco lobbying and politics at the time. Very few studies provide such clear numbers. And that brings us to smaller studies, case reports and single-person experiences. There's no averaging effect in a single person, so if a single person finds a large effect, that's typically pretty meaningful for that person. Also, in contrast to large studies, symptom improvements matter much more to people than proving an exact cause. Let's have a look why small patient groups or single-person data can be so powerful…
It also matters what a study measures. Studies that track real outcomes – so-called "endpoints" like death, heart disease or migraine attacks – are far more valuable than those looking only at risk factors. A risk factor such as a cholesterol level or blood pressure is just a proxy that we believe is linked to a bad outcome. As newer research arrives, risk factors can turn out inaccurate or wrong, while a count of deaths is hard to argue away.
A few well-known risk factors, though, such as smoking, obesity or diabetes, are so well-studied and clearly harmful that there's no point in studying or researching them further. The useful question isn't whether they're bad (we know that already), but how to get rid of them: how to stop smoking safely, how to get diabetes type 2 into remission, or, for type 1 diabetes, which we still presume is a lifelong defect, how to keep blood sugar at a safe level (for example with low-carb dieting).
Case reports, online forum posts, anecdotes, health podcasts (N=small)
In contrast to the above study types, these involve far fewer participants and may have questionable or unknown sources.
Online communities like Reddit are full of short posts and comments recommending this or that supplement. Magnesium, for example, is widely hyped for its calming effect, allegedly helping for insomnia (sleep issues), headaches, mood disorders, and more. Recommendations vary widely on which magnesium salt and timing to use for each purpose.
After reading social media content for a while, you may end up more confused than before. But there's value in it: the ideas might be valid. If some online suggestion worked for others, it could help your symptoms too. Conversely, there's the real risk it makes everything worse for you, or doesn't have any effect and wastes your time. Reaction to certain supplements or medication, or avoidance thereof, can be very individual, ranging between super helpful, useless, triggering a new disorder or symptoms, to outright life-threatening.
How can you tell if online information is safe to try? Look into evidence from professional studies, or take an informed guess. Say a large study says "90% of participants benefited from magnesium for headache symptoms". This doesn't mean you're in those 90%, or even in the remaining 10% of people. Your symptoms and conditions may not have appeared in the study at all. Magnesium might work differently for you, or not at all. The more studies and experiences you read, the better you'll judge which effects are plausible, helping you decide whether to try something. If multiple studies find headache sufferers benefit, trying magnesium makes sense, unless a health condition contraindicates it (discuss with your doctor). But you can't know if it's safe or effective for you just by reading studies. You're guessing at best. More information sources and success stories from patients with similar symptoms may reveal other proven or experimental interventions, medication, lifestyle or diet changes worth trying. Since we don't live for unlimited time, sometimes trying a few things at once can make sense: reducing sugar intake, exercising regularly, taking a small supplement dose for a month? Yes, this could quickly yield positive, neutral or negative results. Your symptoms vary by season or month-by-month? Then you need to try experiments for longer, unfortunately. Ultimately, you need to judge which sources you give some trust, what to try, for how long, etc.
There are also many health podcasts on various topics, often with experts interviewed by renowned podcasters. They can spark good ideas, but typically cover known evidence rather than rare cases.
In summary: ingest all kinds of information without immediately judging trustworthiness. Keep notes of visited links and your own summaries – over time this builds a personal "knowledge base" for each health topic. You'll learn below which online sources to use for studies, case reports, anecdotes and more.
Citizen science (N=small)
The term "citizen science" can mean different things: on one hand, it can mean for anyone in the population to use or provide open, public data. For example, the eBird app tracks bird observations and thereby creates data of the sightings. Scientists and institutions might make use of such data, for example for the purposes of nature conservancy. If you search the term online, you will find many, many projects across the globe.
For human medical health, citizen science could mean individuals running and sharing self-experiments with structured data to support results. This means to track certain variables like sleep, exercise, diet, mood or pathological symptoms. Experiments should change few variables for a certain time, and results should be written down. Citizen science empowers anyone to contribute valuable research regardless of profession or background. Organizations like the US-based Citizen Science Foundation actively work on health science topics and run studies.
This differs from single-person science (N=1) in its sharing aspect: citizen science involves institutions running studies with participants or gathering group data (such as blood tests, filled questionnaires, etc.) to share results. It's collaborative by definition. As a single person, you're not required to share any data, but you still do scientific research on your own health, possibly using others' data too.
Single-person medical science (N=1)
Heard of "biohacking" or "longevity"? These terms are gaining traction but still feel like a niche of few people that are really interested in their health. Don't get this wrong ‒ many people want good health for themselves, do sports, are actively using their gym membership, and so on. But communities actively researching their own health remain uncommon.
The other end of the spectrum: how many people research, discuss and act on their health problems beyond a quick "my back hurts"–"sorry to hear that" conversation? Reality seems to still be that people often rely solely on doctors, newspapers and, in younger generations, probably short-video influencers. We live in environments where doctors typically spare only few minutes per appointment, journalists write sensationalist headlines with distorted facts, and health influencers produce shallow content focused on monetization. These sources rarely show the full picture of what could be wrong with our own, individual health. Can we use these sources better, choose higher-value sources, improve the medical system and add the individual component?
Ask yourself: who has the most time to invest into your own health? You and you alone is usually the right answer.
Second question: who has the most experience about your own health? Same answer.
Third question: who has the most knowledge about your own health? You? Here it gets tricky! If you had enough knowledge, you'd have solved those health issues already. And if your doctors had enough knowledge and input, they would've found solutions too. Knowledge is what you collect while researching factors that influence your health. It's highly individual and can't be compared to others', and how much knowledge you have accrued may be irrelevant since all you care about is solving health issues and improving well-being, right?
But let's go back to having nobody around who was able to invest lots of time, effort, attempts and possible solutions to fix your problems… That's exactly why staty exists: this situation and lack of awareness and interest is not optimal. Taking more care and putting more effort yourself into your own health could have a tremendous positive effect.
To be clear: Modern medicine has come a long way. Doctors in the usual short-appointment setup can do incredible things. Think of back pain radiating to arms or legs. After a few weeks and a 15-minute MRI, a disc herniation is found and known treatments can be started. Countless examples exist for acute, preventative, emergency and other types of medicine that are highly effective. Your health journey should always start with the respective doctor: blood tests, excluding dangerous conditions, imaging where reasonable, referrals to experts and treatment discussions.
If you're using a tool like staty, however, you probably haven't found medical solutions yet – or want to improve areas outside regular medicine like longevity, diet or biohacking. Some illnesses and symptoms are so diverse, individual and little understood that mainstream medicine hasn't fully solved them for most people. Insomnia (sleep problems), for example, comes in many shapes; only certain causes (like obstructed nose leading to sleep apnea) are easily detected. If your insomnia stems from less common causes or doesn't occur consistently, you might run from appointment to appointment without finding a cure. That's where individual data collection and correlations come into play. Fixing your health quickly and efficiently is the goal. By checking your observations alongside medical help and others' experiences worldwide, you greatly increase your chances of success.
Okay, we assume to finally have caught your attention and convinced you that actively being interested in your own health is a good idea!
Here's our vision: in a few years, many people take notes, find causes for their problems and share them online in a relatable way (a data chart or post like "XYZ ruined my sleep, it wasn't screen time, blue light, ABC or DEF"). The more people do this, the more we help each other solve previously hard-looking problems. That's what "science" means: the Latin word "scientia" means "knowledge", and for centuries, the term has meant "having and sharing knowledge" while mankind developed a plethora of incredible things, ideas and, well, knowledge. Sharing is caring in the truest sense. People posting detailed information and data about solved health issues is a countermovement against super-short posts, comments and videos that have become the norm across the internet. Maybe we'll reach the point where illnesses are solved by a combination of highly informed sufferers who personally relate to diseases or symptoms, and modern medicine. A time when patients aren't dismissed as "psychosomatic", but checked for causes inside their body and compared against documented N=1 cases to see which ideas might work.
There's a big downside though: you can't know everything, and doing things alone can be riskier. In biohacking, people love sharing their supplement "stack" – social media posts titled "Rate my stack" show pillboxes, often without any efficacy or risk data from the author. Supplements and chemicals can have strong negative side effects up to life-danger zone. Following only one trend, like taking freely-sold supplements as the only way of getting a few percent better, can lead down a dead-end while the root cause and possible major solutions may (or may not) lie somewhere else. Below, we share examples of wrong conclusions, risks and staying open for new insights, so you don't run into a corner or harm yourself while trying to improve health.
How can N=1 science complement high-quality, large-scale science? It allows finding individual solutions that may not appear significant in averaged values of larger study populations. For example, what if a nasal dilator or strips help a few sleep-deprived people with specific nasal passage problems or apnea, while studies don't strongly recommend it? Such non-pseudoscience solutions should be available and documented even for very small groups. With freely-available information and shared N=1 findings online, more people can achieve better health.
Correlation and causation
"Correlation is not causation" – one of the most important concepts to learn. Science is often inaccurate and rarely provides absolute facts, with very few exceptions.
Basic example: ask 10 sunglasses-wearers whether they get dizziness frequently, and 8 say yes. You've found an interesting clue but haven't proven sunglasses cause dizziness. You've done much less research and data collection than would be necessary to prove or disprove it. Did you ask people worldwide or just at one location? Maybe they all had the same bad hotel food causing dizziness, and sunglass wearers are just more common in beach hotels. Did you ask only in summer or at multiple times? Do symptoms vary throughout the year? Did you collect more info, like current medication, family history of dizziness, sleep quality? Did you try wearing sunglasses yourself? Many variables could impact dizziness, some known and many unknown.
Now that you understood the concept, let's go through some more examples. Some are real and some are contrived:
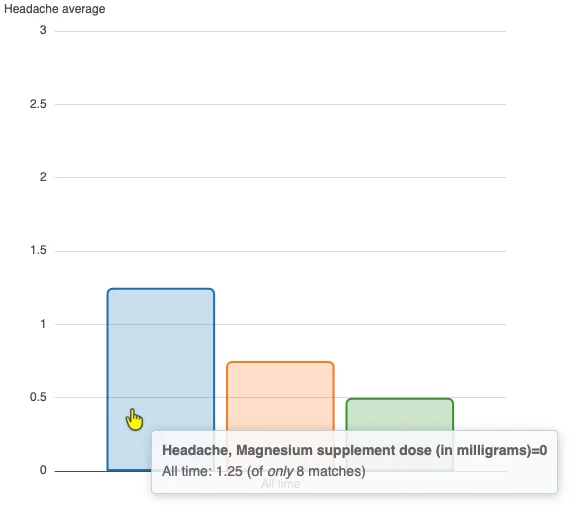
Have a look at this graph. What can you say about the effect on headache in the person this belongs to? Can you state that it helps/exacerbates headache? Which conclusions can you draw about magnesium for yourself?
These things should come to mind:
- No context shown: no time range, patient info, bar counts (how many days the average covers), Y-axis meaning (0-3 scale), or whether this is questionnaire-based subjective data ("headache strength" isn't even mentioned) or some objective measurement.
- The magnesium product isn't specified, only dosage. We can't assume that only a single product was used.
- Underlying data isn't available. You only have the graph without commentary.
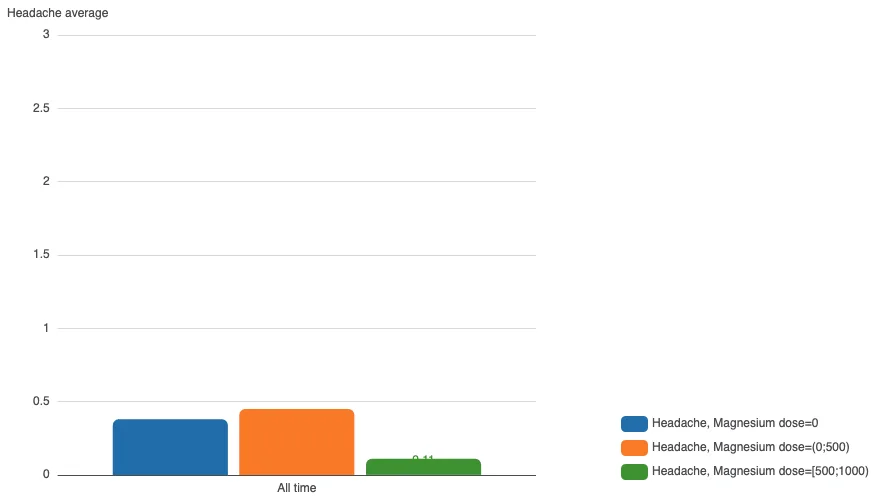
- The low dose (<500, assuming milligrams, unit unspecified) seems as ineffective as no supplement. The higher dose (500-1000 mg) appears to strongly improve headache.
- Was another supplement or intervention tried alongside high-dose magnesium? That could be a confounder.
Imagine getting herpes ulcers ("cold sores") on your lips occasionally, researching prevention and finding echinacea lip balm as proposed solution in a hidden internet comment. You buy that funny, green lipstick and try it. Over the next months, you barely get those annoying blisters – confirmed over a full year, ruling out seasonal differences. Time to tell everyone that echinacea prevents herpes outbreaks?!
So far, so good. One ailment solved. Absolutely nothing wrong with having a working solution. But there's still something wrong with your scientific approach and freely claiming cause-and-effect: you didn't find the actual cause, only something clearly correlated with prevention. Seasonal differences such as high UV light index in summer were ruled out because you tried it for over a year, cool. However, the lip balm has 17 ingredients including unknown amounts of echinacea extract. No way to prove which compound helped. To get closer to a "proof", try less of this intervention. It turns out regular lip balm from typical brands (without that strong echinacea taste that shocks your partner while kissing) has the same effect! Research shows UV light exposure is a strong stimulus for herpes outbreaks. So it's not echinacea, which you found statistically correlated with blister prevention, but the UV protection in many lip products that likely prevents blisters. Do you need to find a true cause relationship here, or the exact compound protecting your lips? Not really. You want a life free from outbreaks and just need to know which (cheap) product works long-term. If you were an institution conducting a large study, things would differ, of course.
The biggest limitation of this study is that it finds an association between current dog ownership, not past ownership, and tracks the onset of disabling dementia over a relatively short 4-year window.
A more plausible explanation for the finding is reverse causation. Owning a dog requires consistent executive function, such as feeding, walking, and basic care. Individuals in the early stages of dementia are often no longer able to manage these responsibilities independently. As a result, many may give up their dogs before progressing to disabling dementia.
This creates a bias: those who remain dog owners are disproportionately healthier at baseline, while those already experiencing cognitive decline are less likely to be in the “current dog owner” group.
In this context, dog ownership may not be protective. It may simply be a marker of preserved cognitive function in the years preceding diagnosis.
Nonetheless, for those of you who love your dogs, keep loving and petting them. There is no doubt in my mind that owning a pet is therapeutic for many things.
In summary, correlation refers to a statistical relationship between two variables, indicating how one may change when the other changes, but it does not imply causation. Causation can be proven through controlled experiments, longitudinal studies, or clear mechanisms explaining how one variable influences another.
Cofactors and why you can't test every combination
Cofactors are a special causality trap: two or more factors you happen to combine, so their individual effects get tangled up. Say your headache is much worse on days you eat broccoli, but also on days with minced meat (a contrived example) – and you usually cook the two together in one meal. From that data alone, you can't tell which one is to blame, whether only the combination does it, or whether yet another cofactor such as a condiment is the real trigger. The only way to get clear data is to separate them: deliberately eat broccoli without minced meat, and minced meat without broccoli, then compare. Even a few weeks may not be enough – the worse headaches could be pure chance, unrelated to these foods and no worse on average over a longer period.
This is also why you can't test everything at once. Imagine trying four interventions against sleep problems: melatonin, omega-3, magnesium, and tryptophan. Recording each as just "taken or not taken" already makes 2×2×2×2 = 16 combinations – and more if you vary the dosage. It's tempting to run each combination for a single day and feel done within a month, but that doesn't work…
That's far too little data. Sleep problems vary a lot on their own, and unknown cofactors push them around too: food, medication, environment, travel, exercise. One day per combination is far too noisy to judge anything. You'd need at least a few days per combination, which can add up to several months or a whole year for this experiment of four supplements.
In theory you'd need a huge number of days; in practice, you do something smarter: you exclude. Over a few weeks, look at one factor at a time. For example, how were my sleep problems on days I took magnesium versus days I didn't (ignoring the other supplements)? If there's no difference week after week, or the results are mixed (inconclusive), then magnesium probably has no consistent effect for you. Consider dropping it from the experiment for now, or for good if you clearly saw no effect. Ruling factors out one by one shrinks the giant number of combinations back to something you can actually reason about. And there's a good chance that none of the supplements help at all, whether alone or combined.
Whether you have the mentioned structured approach of combining the four interventions in this example experiment, or tried certain interventions kind of randomly – on some days yes, on some days no – you can analyze your data to see trends. The "combinations" feature in staty lets you easily visualize the 2×2×2×2 = 16 combinations, for instance in a bar chart. If one of the 16 bars has an unusually high or low trend, consider looking into it more. Bars are shown as half-transparent if you have less than 10 days of data for it. Hover over a bar with your mouse cursor to see how many days of data it has, i.e. how relevant it is.
Of course you could try interventions one after another, not four in parallel as in this example. That makes it easier to reason about results, but takes longer after all to try multiple things that could help. You still need enough data to tell actual effects from non-effective treatments.
Absolute and relative percentages
Simple example why you critically need to understand the difference: a study comparing flu rates between vaccinated and unvaccinated groups found 5 per 1,000 vaccinated individuals got the flu vs. 10 per 1,000 unvaccinated. The absolute risk reduction – the real-world difference – was just 0.5%. But relative risk reduction showed the vaccine cut flu risk in half (50%). The relative percentage makes the vaccine seem highly effective; the absolute percentage shows actual population impact, which can be much smaller but still meaningful for public health decisions. Would you take this vaccine, given barely any benefit? (This is a fully contrived example, and the real world has better vaccines!)
Here's another one, for the fun of it:
Now that the basics are clear, look at Zoe Harcombe's 2015 post about the WHO declaring red meat as possibly carcinogenic. She critiques the bad science. Give it a read and see if conclusions make sense to you. Any points that aren't fully fact-based? The percentages should now be clear: absolute cancer risk difference is negligible. Also: let us stop grouping unrelated things into single categories. Red meat is the raw part of an animal (minus minor processing like removing blood), while processed meat can contain or be rubbed with dozens of ingredients, and even be high-carb such as a breaded steak. They're absolutely not the same, yet science often treats them as one category in food questionnaires, making results useless. Don't repeat this mistake in your own data collection. You can group cheese, cream and milk as "dairy", but also track each separately since the body reacts differently to these foods because they are different.
Science failure stories
The percentage story above was hopefully eye-opening. But science and journalism don't just overstate results. There are major historical cases of results that were wrong, fake or, in the below example, hidden in the cellar.
Ancel Keys proposed the diet-heart hypothesis in the 1950s: high blood cholesterol supposedly causes clogged arteries and heart attacks through fat deposits. Even today, people demonize and overgeneralize cholesterol while science has long advanced past this disproven theory. His stubborn defense against contradictory data is too extensive for this article; read about it in The Big Fat Surprise or watch Dr. Paul Mason's lectures such as The corrupt history of the food pyramid. 21st-century research not only disproved this, but created new fields exploring better explanations for atherosclerosis and heart disease, leading to research and use of low-carb diets and more predictive risk markers.
Some scientists don't report "negative" results well or at all. The Minnesota Coronary Experiment was meant to prove that lowering cholesterol (by using for polyunsaturated fat in the diet) reduces heart disease risk and mortality, but its data was "lost" for decades on storage tapes in an author's basement. A persistent researcher rediscovered it, and re-evaluation in this 2016 paper didn't support the claim. In people over 65, decreasing serum cholesterol had a "robust association" with increased death risk. No difference at younger ages. The health impact of this incorrect theory persists: people still, in the 2020s, buy low-fat alternatives, get prescribed cholesterol medication without strong indication (note: there are such indications in certain diseases!) and trust industrially-altered fats like margarine. Understanding where to get the "right", latest information is key in this world where the internet is exploding of mixed recommendations about essentially every health topic.
Read about these topics yourself – this page is neither medical advice nor a complete assessment of the topic! Just think of the consequences of someone reading the above paragraph, turning their world view away from "cholesterol is bad" based on this summary, only to discover they're one of 0.04% with familial hypercholesterolemia, a genetic and individual condition where elevated cholesterol can be life-threatening. You can't adopt a new worldview from a short scientific history summary. You need to do the full reading. Likewise, don't believe newspaper claims just because it's your favorite paper. Do your own research on every topic.
Why N=1 science is easier and faster than "real science"
Strong correlations and symptom reduction are enough for N=1 data. No need to prove causation, no need to convince other people. This differs from "anecdotes" – stories about how a health issue probably improved, given subjective observations but often no clear data. N=1 "hobby" scientists write down and analyze structured data to test their hypotheses, sharing numbers like "before trying X: headache every Y-th day; after: every Z-th day." The primary goal isn't telling others (though that's valuable) but observing and solving your own health issues first.
Getting there takes time: 10 days of headache strength and magnesium intake data says very little about effects. With years of data, an overall average may be too simple – check per-month or per-week statistics for mixed or varying outcomes. Once you reach certainty, you've likely found significant health improvements and can consider sharing your story (more on reasonable sharing below).
If you instead were a participant in a middle or large-scale study, solving your health issue isn't guaranteed: if you're in the randomized control group (unaware that you are), you get only the placebo effect and no real treatment. You can't choose interventions, and they aren't tailored to your health. Studies are limited in funding, so don't expect detailed individual tests (blood tests, investigative appointments, cofactor observations), but rather one method across all participants. Results may take months or years depending on study size and type. If you're in the control group, that's when you'll discover this "wasted" time. Various biases exist too – publication bias, financial influences – meaning study data can never be fully trusted. Your own data is different: it's fully trusted; the only untrustworthy part are your potential misinterpretations of it.
This view of large studies is harsh, but you should try newly-researched treatments when known ones fail. It depends. You may read on this page that we assume you'll actually find solutions for most health problems by doing N=1 research. Well, that's not a statement one can make. What we can say: people often miss options until they deeply explore information sources presented in this guide. If someone only visited one doctor who shared main medical guideline ideas for issue X, remaining well-known options may never have been mentioned or tried. Short appointments, limited testing (missing important blood markers for cost reasons), or not following latest science and anecdotal solutions can cause oversights. That's why the diagram at the top of this article shows how the medical system, different study types including individual self-study, could together prove as the best possible care. Believe it, or not – in the end, the only thing that matters is improving our health.
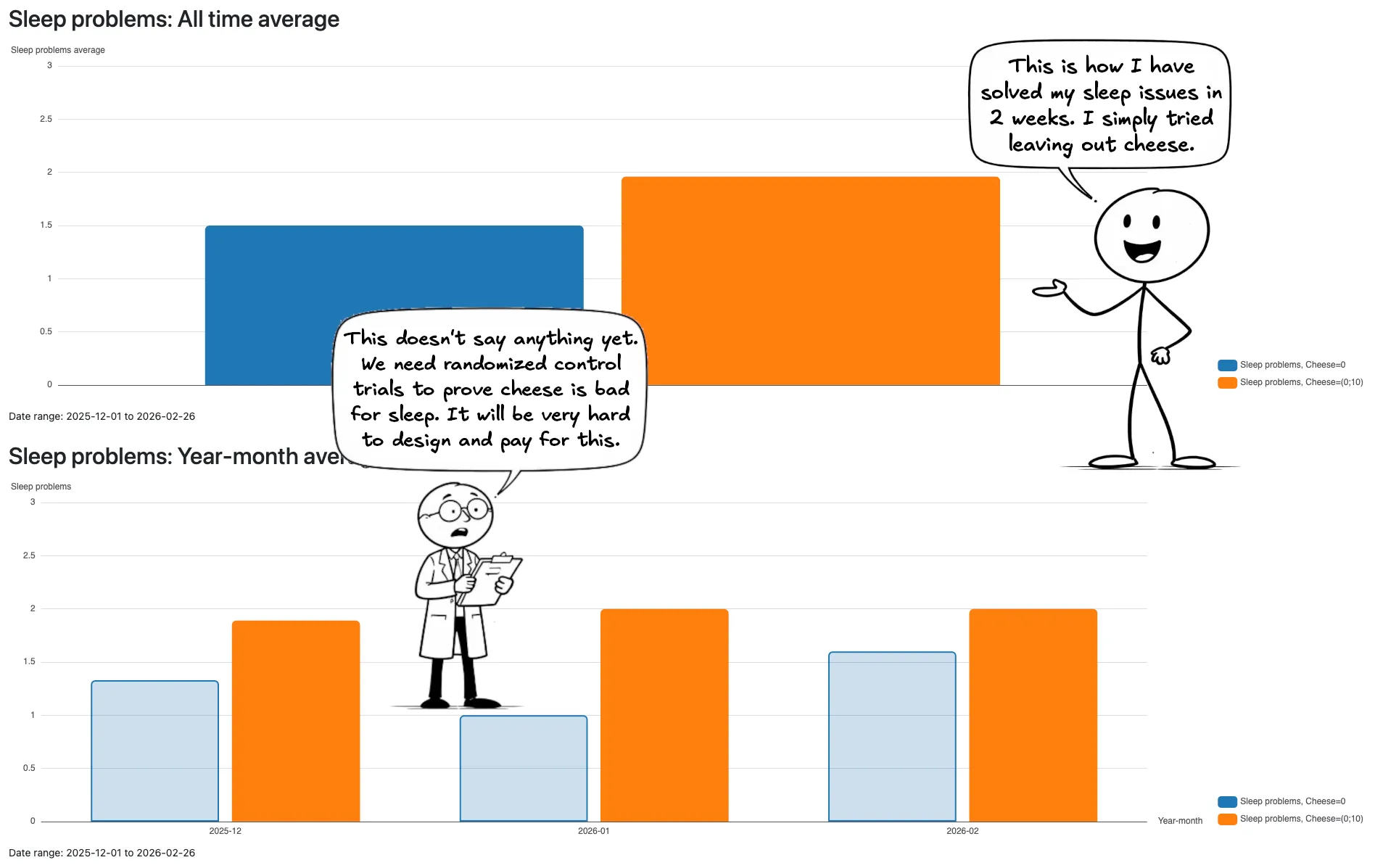
In the cartoon, the data, showing 1+ portions of cheese are consistently bad for sleep over 3 months, is real. The "I solved this in 2 weeks" part is contrived. It can be as easy and fast as in this example, given you find these clues and decide to leave out a food item temporarily. The cartoon simplifies: it doesn't show the following months proving whether sleep trouble mainly came from cheese. This also doesn't prove scientifically-relevant points like whether tyramine content, a specific cheese type or something else helped. The point is no RCT is needed to help this single person.
How do I find out which interventions are worth trying?
Writing down symptom strength is easy. You can judge and write "headache strength" in a spreadsheet, every day, without a problem. The hard part is getting started with interventions to alleviate symptoms. We'll cover information sources later; this section covers choosing what to try next.
You can't easily make choices – that's why it's called "science". Health has an incredible number of possibilities, sometimes probably even no known solution at all for rare diseases. At first, you don't even know what options exist. "Choice" implies selecting from known options, but medicine is often a guessing game without a menu. Most likely, looking at probabilities makes sense: headache with typical migraine symptoms suggests migraine over tension headache – try a fitting intervention accordingly. If you can fall asleep at night, but wake up often and cannot fall asleep again, you will not search for "sleep onset problems", but rather for "sleep maintenance problems". Let the rough observations of your health problems guide your search terms and forum questions.
Internet posts and comments often repeat each other people's opinions and attempts. Seeing many similar views doesn't mean they're the majority experience.
To gauge an intervention's chance for success, check if it was studied, how safe it is, and whether studies show percentages of people helped or if results apply only to certain subgroups. Rarely mentioned interventions are still relevant but might be placed further down on your list of things to try (principle: try the obvious first). You can never know exact chances regardless of reading – but you can try things out.
It's also important not to draw false conclusions on your own. For instance, thinking "I eat meat and healthy foods, so I can't be iron-deficient" is extremely short-sighted. Without a recent blood test, you just can't know and might have a deficiency. And even values that are "still in the normal range" could still cause certain diseases. For example, with the restless legs syndrome (RLS), the recommendation (and first-line treatment) is to raise iron levels to a higher level than the norm.
For supplements or medication: understand how they work. Some materials are buffered by the body (e.g., vitamin D) and take longer to show effect, based on the accumulated level in the body. Others only work while blood levels stay high. For example, "stimulant" medication like Ritalin works for a known number of hours, requiring daily dosing. Formulations of pill, powders and other forms vary widely: sustained-release (retard, extended release/ER/XR) vs. immediate-release, oral pill vs. liquid vs. intravenous. Supplements are typically less quality-controlled than pharmacy medication and often sold without prescription. Some lack safety info or studies showing a clear effect. Some are highly effective, some dangerous, possibly varying by individual. Read official or studied information about expected effects, side effects, risks and time-to-effect. Don't stop at the package insert. Read others' experiences too, especially for your health issue.
Don't fall for pseudoscience. Particularly homeopathy, a rip-off since the 18th century. Tiny sugar pellets ("globules") mixed with an active ingredient "potentized" (diluted to barely detectable levels) can't have more effect than placebo by definition. It's never worth tracking and analyzing data for such "snake oil". You'd likely become just another person spreading false information based on false beliefs.
Many doctors still prescribe homeopathy in many countries as of 2025, sometimes even wished by patients based on stories they heard: "The globules helped our baby against teething pain", families might claim. Teething is highly individual – some babies are born with teeth out, others get them well past one year, most fall between. About 80% of infants experience symptoms like increased biting, irritability, salivation, gum rubbing and mild temperature elevation. Prevalence even varies by geographic location. This many variables, plus families not comparing globules against a "control child", makes such claims impossible to verify without a study or identical twin comparison. Pain and other symptoms can't be precisely measured – parents or investigators must assess them subjectively, which is extremely inaccurate. This same problem exists in fields like ADHD symptom severity evaluation based on parent and teacher questionnaires. Without biochemical measurements, these fields remain inaccurate. Going back to teething: pain and symptoms may come and go, occur rarely over a few months, and therefore cannot even be assessed reasonably in N=1 science, nor can a claim about homeopathy's effectiveness be easily verified without a very good study design and many participants.
The heading was how to find interventions worth trying, but we haven't given exact instructions yet. Sorry, that's hard to do generally. Check relevant online sources (explained below), read widely and make an educated first selection from the collected knowledge. We may add guides for certain health issues in the future, depending on available time (staty is unpaid volunteer work!) and potential liability concerns. Send us feedback if you think such guides would be valuable and for which topics.
Why do all this? Is it worth it?
Does writing down "headache strength", "how much of medication/supplement X did I take today", "what were my blood sugar and ketone readings today" and other data into a spreadsheet result in improved or resolved health issues? Yes – though results vary since people are different. Some face difficult health issues, some may not grasp statistics well enough for good decisions, some might give up. As author of staty, I created this app solely because data and statistics help – it was published after years of work because I'm confident it will help others too. There's no guarantee you'll find solutions for your specific issues, of course.
To "prove" that, let's look at improvements I achieved years before publishing staty, and what would have happened if I hadn't become a hobby scientist:
Memories of migraine in my youth: Vomiting through nights as a kid. Years later, as an adolescent, after school, I'd often stay in my room with blinds closed, wanting to lie down and "sleep away" the pain – though I couldn't sleep. No diagnosis despite clear symptoms. Few doctor visits or parental attempts to fix this life-shattering illness. Useless attempts like aspirin or coke never worked (or may have aggravated it, who knows).
Later, after losing some naivety, I started tracking headache strength daily. At that point, I had a headache every third day, full migraine every 14th day. Not as bad as in my youth, but still debilitating because even the moderate pain affected my well-being immensely.
Stop. Now imagine I never wrote down headache days or researched interventions. How would life go? Either nothing changes and I'm still sitting in pain every third day. Or an odyssey of doctor appointments, maybe some improvement from long-term treatments like modern preventatives or botox. Chances of finding and solving the cause? Zero. Getting standard medical care? Sure. Optimal solutions, that is, zero migraine? Unlikely. I only know that now, after having those solutions, realizing standard medicine wouldn't consider salt supplementation or the ketogenic diet in the early 2020s when I started these health efforts. Another alternative future: like in childhood, trying things that "seem to" work and falsely believing them. Believing in french fries and coke, magnesium, vitamin D, soda, alcohol reduction – attempts that eventually brought minor or mixed improvements, if any. That would have meant relying only on feelings and believed observations, without journaling or doing even simple statistics. Another problem that would have occurred without data: months of extreme dizziness, to the point that I feared driving my car. It came from excess vitamin D in the body, fading only weeks after discontinuing its intake completely. Vitamin D is buffered in the body. It came from 2500-5000 IU/day supplementation. I repeated this "involuntary experiment" with 1000 IU later, a dose documented as safe for normal adults. Even that gave dizziness, and my data showed sleep trouble correlating exactly linearly with daily vitamin D dosage. This made me eventually give up on this generally-recommended supplement. Just imagine me taking months or years longer to figure out the cause for dizziness and parts of my insomnia.
It luckily didn't happen that way. I did write down data, find tiny improvements and lots of non-solutions among well-known, studied supplements (CoQ10, magnesium, etc.), understand my triggers better from data and closer observation. After some years, I did discover salt supplementation as a major intervention that worked for me. I did get annoyed that this knowledge existed for 10 years but I hadn't found it online yet. Lastly, I did invent staty for myself and make it available to others – all while hitting other extreme health issues and personal crises. Every single minute of reading studies and anecdotes, developing this app, writing this guide, solving health issues and trying to help others was worth it.
- IED, a mental health disorder: Histamine overload, uncontrollable anger, bad behavior towards others. This would have led to me being alone eventually after losing everyone. But I found the biochemical source of evil, excluded high-histamine food items for a while and, despite not finding the root cause, have seen tremendous improvement.
- Sleep trouble: worsened significantly in one month with no clue why. It started one week before a trip to a foreign country, and I don't remember any food poisoning or other influences. Without data, "listening to my body" would just result in silence and I would have no way forward. I didn't solve this one yet, but managed to rule out lots of factors already, such as the oh-so-often mentioned evening screen time and sleep hygiene, allowing me to focus on others.
And is it worth reading up about new health information and science all the time, reducing your free time that you'd rather use for fun activities? Well, it can become a real hobby the more you read and dig into information that is already out there. But yes, it can help. Here are more examples to showcase how N=1 can have a positive effect:
Health professionals often spare only few minutes per appointment. Their experience with your specific symptoms varies widely – general practitioners must know about thousands of conditions and cover the masses. To direct you to the right specialist, a general practitioner already needs the right clue. That "system", used in many countries, sometimes doesn't work, especially for unclear symptom causes but also others.
Here's a real, anonymized case: a boy gets referred to the child doctor for a blood test related to symptoms of ADHD and restless legs. Particular nutrient checks such as iron storage were added to the laboratory panel due to those symptoms. Results come back to the child doctor – who is a general practitioner and not trained in neurology. He tells the kid's parents "all values in the blood panel are good, best regards" and that's it. One parent has familial restless legs syndrome and knowledge about its genetic inheritability, checks the blood results and sees several, glaring iron deficiency markers. The child doctors, due to missing knowledge, refers onwards to a child neurologist. And it turns out the neurologist has much more experience with epilepsy and is not at all familiar with the restless legs guidelines. The boy eventually gets treated for iron deficiency anyhow, as would have been the first-line recommendation in medical guidelines, based on blood levels.
This story is here to showcase solvable gaps in the medical system. In this case, just a lookup of the national RLS guidelines, even if only summarized by some AI search engine, would have provided the necessary start to give the blood levels a second look and consider iron deficiency and therapy which were clearly indicated. Latest at the neurologist, patients would expect something like that. Yet it didn't happen in this story. Indeed, technological support in practices is still missing a lot. Many countries already use a system of requiring or incentivizing doctors to take trainings, and they often happen in certified online trainings of different depth and quality. Despite such efforts, for example, knowledge about the restless legs syndrome (RLS) still didn't arrive at the doctors in the story, while experience with epilepsy, another neurological disease, seemed covered much better. Why is that? Compared to epilepsy, RLS has higher prevalence in children and adults. So is epilepsy preferred in study curriculums and trainings because it's more dangerous, while RLS is considered a problem for sleep and life quality, but not a health danger? Shouldn't specialists be aware of the basics of all highly-prevalent diseases, or at least be able to look up guidelines?
We're going too far into what we cannot easily influence as single person or as parents unless we become politically active. And the above case only represents some downsides, while the medical system in developed countries can work very well in many cases. The important piece is what you can influence. We don't need to fix the system to improve our own health outcomes. Informed patients ask better questions, get faster answers, can see connections to other disease cases they have read about, and have a higher likelihood to understand symptoms, disease and causes themselves. They can leverage all possible information sources, not only appointments, to their advantage. Compared to doctors, patients only need to care and learn about themselves, not about every major disease on the planet, so it should be much easier than medical university to get started on this. Wouldn't it make sense to have illnesses investigated and solved not only by scientists and doctors, but also by highly-informed sufferers of the disease themselves?
Understand that RCTs and other high-quality studies won't and often can't directly provide answers for your individual problems. Here's a good, short explanation why N=1 science makes sense (Chris Masterjohn), and here a detailed essay what N=1 science can do (Nick Norwitz). Both of the authors are researchers who focus on metabolic health, longevity, and more health topics. They know their stuff, and use their knowledge for themselves as well, while also being so nice to share well-researched information with others.
Quoting Nick Norwitz:
N = 1 science captures the philosophy that every human being has the power to apply the scientific method to their own life by:
- Identifying an element of their health they want to change
- Hypothesizing about what intervention(s) may impact that outcome
- Implementing the intervention
- Assessing their own outcome data (objective or subjective)
- Repeat, ad infinitum
N = 1 science empowers people to become “citizen scientists,” experimenting and refining their health choices to find what works best for their own bodies. This self-application of the scientific method to one’s own metabolic health journey, if properly executed, almost guarantees long-term success.
How and what to write down in your health spreadsheet?
This will be covered in other guides in detail, but let's look at the basics:
- Which symptoms to write down? All bad symptoms should be written down. Some obvious ones: sleep problems, tiredness by day, depression, anxiety, concentration or productivity (at work, at home), headache strength.
- Which related things to write down? In staty, both symptoms and other numeric or non-numeric data are called outcomes. They might be anything: the brand of toothpaste you use, whether you did a certain hobby or sport, at which hour your headache started. Think of questions that you want to ask your data: if you want to fix your insomnia, you must write down the symptom "sleep problems" and anything that you want to check that could have an effect on it. If you want to know "Do fights with my partner cause bad sleep for me?", then you'll need to put "Arguments with my partner" into your spreadsheet. Also, always try to write down things that are obviously related in the general population. For sleep problems, that might be: did you take magnesium or other supplements on that day (and when), did you do sports (and when; late sports can be really bad), how long have you been in sunlight during the day, did you take caffeine (from tea, coffee, chocolate, supplements) or other stimulants, intake of medication, etc. At some point, if the data analysis shows no difference for some of those, for example more or less sunlight doesn't affect your sleep at all, you can still decide to no longer write that down. But you cannot decide later to check sunlight as a factor if you never wrote it down. So writing down more possible factors is better, for a while.
What exactly to write down? Which number scale makes sense? The easiest and most common examples are numeric data: if you want to write down the symptom "sleep problems", a higher number is worse. Large-scale studies or doctor appointments sometimes ask for pain on a scale of 0-10 or 1-10. Were you ever able to tell apart a 5 from a 6? Likely not. And that's why those scales are very inaccurate and we don't recommend using them for your own data.
In the example, you should define only as many different numbers for the "levels" of sleep problems that you can differentiate. The author of staty successfully uses the 0-3 scale. It has 0 (zero), which obviously means great sleep, not too short or too long, no problems getting out of bed or falling asleep. The number 1 means mild problems such as waking up too early, feeling a little groggy in the morning. The number 2 means moderately severe issues like failing for a longer time to fall asleep, waking up in the middle of the night and not sleeping well afterwards, not feeling rested in the morning, trouble getting out of bed at a reasonable time. And 3 is the worst imaginable: feeling of not having slept at all, tried multiple times in or out of bed to become sleepy and fall asleep, woken up multiple times or not recovered on the next day at all.
For any scale, at best, you are able to describe each number with words, and even write down the description in your spreadsheet in order to stay consistent over the years (use the "Comment" function if your description is very long). Note that the scale 0-3 has a "middle". Zero is special, while the others mean low/moderate/strong sleep problems. Having a middle item can be easier to judge.
Only using a 0-1 (no or yes) scale is not recommended for symptoms that vary in their strength. Think of headache: a light headache onset is tremendously different than a full-blown migraine attack. If you only entered either of these headache strengths as the number 1, your data won't tell you any trend of the headache strength, but only, to some extent, about frequency (how often a headache occurs). The 0-1 scale makes sense only for "yes/no" entries such as "Did I read a book today?" or "Did I sleep at home today?". These number scales (scores) are easy to use, and explained in more detail, in the standard formats guide.
- Why can time be important to write down? For example, sports in the evening is known to hinder sleep. But just because something is "well-known" totally doesn't mean it's true for you. By writing down something like
15:30,running, you can analyze the effect of early vs. late sports on sleep or other outcomes. Or it might be interesting when your headache started, as it might be triggered by food, low blood sugar, low blood ketones or something else for which you are also writing down the time. - Non-numeric entries: These can make sense if a number cannot be assigned. Imagine you're analyzing whether a certain toothpaste brand has an effect on how often you get aphthous ulcers in your mouth (real example! – SLS and other ingredients are relevant here). In this case, just write down the brand(s) you used on each day. staty can still use these "text values" in analyses.
- Make it easier for yourself: Writing down anything day after day takes dedication. Try writing down your water intake for a few days, consistently and exactly. Tried it? Noticed something? There's also strategy involved. It's much easier to write down water intake if you only drink from a 1 L bottle rather than 250 ml glasses – you can't really miscount a full 1 L bottle?! Or one of those huge bottles with markings for up to 3 L, not requiring you to count glasses or bottles at all. If you don't have time to open the Google spreadsheet, either on a computer or the phone, there's a trick to still note something down: use the notes app of your phone, or just take a screenshot of your phone screen and add a note there – this it will automatically include the day and time.
- What not to write down? Things that aren't changing daily, such as your weight, scores from a psychological questionnaire (examples), or long-term blood sugar value (HbA1c), could be interesting for you to track in a spreadsheet, but are hard to analyze because you just won't ever have enough data to answer questions like "Is magnesium supplementation good or bad for my weight?". The same applies to very rare events: Think of someone who gets a strong headache twice a year and is headache-free on all other days. If that person is lucky and wrote down the potential triggers, there's a chance to find the relationship (real example: dairy causing headache). But if the headache trigger is unclear, it might take decades to find the cause and having to write down `Headache strength = 0` for 363 out of 365 days of the year isn't worth it – that's on you to judge. Some things can change multiple times or continuously during the day, such as blood sugar or blood pressure. Writing down a few instant values could make sense to get an idea of your daily average. As example, the author of staty writes down 2-3 blood sugar and ketone readings per day. This allows learnings about which foods trigger blood sugar spikes, but also enables him to analyze questions like "What's the average headache if my blood sugar has risen above 150 mg/dl in at least one of today's measurements?". You may also find that some things turn out as hard to measure, or unmeasurable. For example, if you can't distinguish between "regular thoughts" and "racing thoughts", simply because your brain thinks of random ideas all the time, then how are you going to write down "Strength of racing thoughts" as a symptom? You should always have a reasonable scale defined for such cases, as mentioned above, or else your data will be inaccurate at best. If a value can be calculated, don't write it down. Instead, use the Google Spreadsheet features. For example, if you write down how much fat/protein/carbohydrates you ate on a day, it doesn't make sense to write down the "keto ratio", but you can just use the formula `fat / (protein + carbohydrates)` to auto-fill it into your spreadsheet if that's what you want. Or if you don't want it visible in your spreadsheet, and only want the keto ratio for analyses, staty can do this calculation for you by adding such a step. Why avoid all these? The less time and effort you need every day to fill in your health data, the more likely you'll do it over the next months and years, and that is critical to get results out of it. Missing a day here and there, and the data becomes useless. For example, if you write down headaches on 20 out of 30 days of the month, calculating the average could give a totally wrong result because the values of 10 days are unknown.
- Unsure whether to write something down? On the other hand, if you think something should be written down as interesting outcome to measure, don't wait, and start immediately! It may prove important for your health and without the data, you'll be screwed once symptoms get stronger and you cannot correlate it with anything you changed or did. Example: I thought of writing down what I eat for a long time, but because the effort is so high to get the macros (calories, fat, protein, carbs) from each food item's package into an app or some calculator, and eventually my spreadsheet, I held off. Luckily I finally did that, culminating in me finding and treating a biochemistry-based mental illness which was in fact easy to solve. I realized that only writing down food ingredients would have been enough. Different foods is very likely to have at least minor effects on your health, through various pathways. I continuously tried to make it easier for myself since the effort of writing this all down was so high – in this case, I added a half-automated way of calculating my food totals and writing down ingredients.
How to find good information?
You finished the first step: understanding what kinds of studies exist, from the above descriptions. Note that you should definitely read a lot more information about the above and not just this article to provide you all necessary knowledge. Go to other definitions on the internet, join and read posts in communities such as Reddit: This curated list contains symptom-/illness-specific subreddits (you're not familiar with Reddit? those are just "forums"). There are also special forums: r/Biohackers is full of people who love supplements and other means to find improvement for physical and cognitive performance, not typically for specific symptoms, but rather for general longevity. Asking your own questions in a reasonable place makes sense.
Social media posts and comments are usually short and unfounded. As reader, you'll get biased by what you're reading. You can't take statistics out of it: If yu continue reading comments about the ketogenic diet like "You don't need to measure ketones, you'll feel when you're in ketosis", you might just take over this opinion without verifying it for yourself. People often just copy opinions from each other, leading to a large number of such comments while the fact might be totally different. My migraine is gone when I'm in ketosis, which I only see from my data, not from feelings. That's how I am. I can't listen to my body so well that I "know when I'm in ketosis", so those comments of other people are irrelevant and not true for me. From commenters that don't provide data, here for example experiences about blood ketone measurements, we don't know if those people are even in a ketogenic diet or just get their reported benefits in another way (such as weight loss, supplements, other activities). Of course, unsurprisingly, measuring meaningful levels of nutrients or bodily energy sources in your blood can make a lot of sense, especially if they're well-known to correlate with certain illnesses! Everyone is different, so all online comments must be viewed with both caution and open mind for the possibility that a comment could be both true and false at the same time – true for others, false for me, for instance.
Bias is a large problem. Even heavily downvoted online comments could have important information. You must be able to tell apart "biohackers" (influencers who sell or get money from products) from "biohackers" (people doing experiments and sharing experiences, however sadly often without numbers or significance). Especially on YouTube, Twitter/X and other monetized platforms, there are many influencers who in some form make money with their health tips. If you find someone adding new posts or videos several times a month, check more closely. Someone who writes about 100 health topics isn't as trustworthy as an expert in 1 topic. Someone who sells a book about a topic may have clear bias to post a lot of unhelpful stuff about the topic rather than helping sufferers. Almost nobody provides information "for free". Since I like the ketogenic diet, let's use this example one more time: try to find actual, clinically applied keto meal plans with a therapeutic ratio of 4:1 – you'll barely find anything apart from some generic, useless recipes that often don't even match that ratio, or the typical info about the ketogenic diet which has been copied a thousand times across the internet. Keto coaches, doctors and clinics get money by treating patients with such a therapeutic diet, and in many it really helps, so don't expect this (yet) to be out on the internet for free. You'll find more information in paid books of true experts, but still might not get the full details as used in clinical treatments.
There are also sources that might be "in the middle" between trustworthy and strongly biased: do you trust Andrew Huberman who's sponsored but very likely has great intentions with his podcast about various? On the other hand, do you trust a migraine researcher who sells a supplement that's supposed to prevent migraine (MigraKet, later renamed to Brain Ritual)? Well, consider the risk of not trying their suggestions. If you don't want to buy and try that expensive migraine supplement, fine, but the idea behind it – the ketogenic diet – is easy to try and well worth the effort. I'm down to zero migraines while on ketosis. For that researcher whose name isn't important here, I can say I'm happy for her to make some money as a Thank You for spreading the word how this diet can help prevent migraine. Still I won't buy the supplement because it's expensive and contains too many ingredients that don't relate to the ketogenic diet at all. Also, check the bias of study authors. Those aren't typically mentioned openly and honestly in the publication, either because people are lying or the bias didn't exist yet at the time (such as founding a company, finding a sponsor or counseling some related company later in time). Just think of the first clinical trials of COVID vaccines – many people mistrust those papers since the companies directly executed the studies and it's never clear whether misconduct or data forgery was in play. (This is not a comment to discredit specifically those studies. No opinion or proven stories about the COVID trials are stated here. Specific health areas are not the topic of this article.)
As mentioned before in this article, you're advised to write down your findings about a topic in a "knowledge base". A simple Word or Google document, or just a text file, is enough to start with. Unless your brain has a very good memory, this is the best way to remember and later read up about your summarized findings about some topic, at best including links to the sources (scientific papers, online forums, videos, blogs, etc.). Over time, you'll create your own view about the topic, probably also supported by trying a few things that you found and which outcomes or non-outcomes those experiments had.
Look at the obvious stuff. You're interested in your own symptoms of brain fog, being unconcentrated, nervous? And you know that a family member has ADHD, for example? Well, just look at the well-known fact that these diseases are highly genetic and therefore your risk is high to have it too, to some degree. Another example: you always had this feeling that cow milk might trigger a bloated stomach for you, so why not write down milk intake and how strong your bloating is on each day, and then look at the correlation after a while? If results are unclear or mixed, it might just be something else and you can replace the original idea and maybe look at other foods as trigger.
On the same note: listen to people close to you, even if you don't want to accept a painful truth or they're hurtful when talking about you. This is especially important for behavioral and mental health symptoms. Have a look at Kanye West's apology for his strange behavior, all based on Bipolar Disorder as a clear explanation. It's very hard to accept the possibility of being ill, but from then on, things usually only get better. If someone repeatedly tells you about your bad behavior, they might be the a**hole, but they might as well be right. For mental health topics, often it's both. That's because the huge stigma and very little knowledge in the general population so your family or close people might rather argue about it than help with solutions. Consider anger, irritability, brain fog, sadness, mood swings, restlessness, memory trouble and other mental or behavioral symptoms as something that you can easily write down, for example on a scale of 0-3 (for example: 0=all good, 3=uncontrollable anger). And consider your body biochemistry, diet, and also your environment (family, colleagues, job) as influences for which you may want to write down some numbers as well. Food is a big topic for mental health as we know nowadays, but it's definitely not the only one.
Here are some concrete sources to use:
- PubMed: The world's central database for scientific publication listings, and often well-formatted full text, if available. Don't be distracted by it being a US government official website. It's the de-facto standard for science. Remember that no study is by definition trustworthy. Watch for bias, bad design, fake images, other publications of the authors, and in general read some articles about "how to read a study" (this one is good). Mind that other science databases exist as well.
- Google Scholar: Not a database like PubMed, but Google's great search engine applied to such scientific databases. They also added an AI mode (experimental, under "Labs" as of mid-2026) that answer questions and prompts by looking mainly into scientific resources.
- Not all scientific publications have their full text published. There are ways to still access them. Some public libraries offer access to certain institutions, for example through their online catalog. Students and university members or alumni may have such options, too. And there are some "inofficial" ways which can't be named here. Sometimes, you find excerpts or figures of studies referenced in social media posts of experts who have full access. Try searching for the study title and authors, for example.
- Medical guidelines: Search for "<symptom or disease> medical guidelines" and you'll find international, country-specific or institution-specific guidelines for your topic. Often, as science advances and the guidelines get updated every few years, the various guidelines across countries are quite similar in their content. Read about which diagnostics and treatments are usually done first, which alternative or off-label treatments and medication are presented, what their efficacy and risk is, which diseases can be confused with the one you searched for ("differential diagnosis"), and so on. This is essentially what doctors in that area should know and follow (but not always do; see stories in this guide).
- Reddit: health subreddits list, search filter for subreddits (example search for "headache"). By joining a subreddit, you'll get relevant posts on your home screen regularly, which can be a good idea next to asking your own questions.
- Twitter/X, Bluesky, YouTube (not shorts; therefore also not TikTok!), podcasts: Follow experts in the health area that's of interest for you, and check out their old and popular posts, too, instead of waiting for new content to arrive.
- Google search: If you know well how to use a search engine, this can spit out great results. Mind that the top results may not be the best results. By adding query words like "study" or "research", you might find more sophisticated articles compared to the clickbait, "Top 10 things to help you sleep" type of content.
How to find bad information?
We've already covered above how to find information, evaluate bias, judge online comments. All of those sources are good information to read. Even if you don't believe some untrustworthy online comment, it's good to read it just once in order to know that some other opinion is out there. When we talk about "bad information" here, we mean stuff that's plain useless and not worth investing time. Of course, do your own judgement. This is just food for thought and we only try to save you some time. Just a single health topic can take years to fully read up about and find out which data and interventions might help you improve your health, so you want to look at the most relevant information you can get, in the time you have available.
Wearable devices and health apps: Do you think you can get any benefit from app findings like "There's a new trend in stairs climbed. You did 4% more than last month."? Most metrics that a watch or fitness band can collect isn't helpful either. A few of them could be interesting: HRV, average heart rate and estimated VO2max for sports and recovery, steps per day for overall health. But in all seriousness, if you're a user of staty, we guess you don't want to analyze your sports performance (you can though!), but are looking into real health issues. People also believe that devices can track your sleep. To some extent, they can, but it's mostly about heart beat and movement, and therefore also total sleep duration (namely the time you stayed flat and didn't move much). Devices can't tell if you subjectively felt like not sleeping at all, had trouble falling asleep, or woke up exhausted. While testing a pricey, modern Garmin smart watch, as an example, I got a sleep score of 82/100 – a pretty good value – despite waking up around 02:15 AM, unable to get back into sleep, witnessing everything around me for the next hours until I managed to creep out of bed, feeling totally wasted (no alcohol or caffeine involved). The reason is that the software mostly interprets my little movement and "sleep time" of 8 hours as "good, uninterrupted sleep". After writing down the device's sleep score for a few months, I noticed that it's absolutely not helpful or in any way correlates with my subjective score (I'm using 0=great sleep 1=slightly too short, fell asleep a little late, woke up a little early, 2=worse and feeling quite exhausted in the morning, 3=couldn't fall or stay asleep, woke up at night without ability to get back to sleep, very groggy in the morning). Other outcomes correlate pretty well with this subjective sleep score of the previous night, while the device data was totally useless. My personal suggestion therefore is to reasonably think about what a band with just a light, movement and maybe GPS sensor can really accurately track. In my opinion, they're great for sports, position and movement tracking, somewhat-exact heart beat, probably HRV (not sure yet about this one), and all their "smart" properties like interacting with your phone or allowing contactless payments. For health, they're of limited use.
Reading only in your own language: If you don't read science in English or other worldwide languages, you rely on minority reporting and miss out on probably already well-known science. Expect that leading researchers in a certain field almost always publish in English. If you're not good in reading or listening to English, Google Translate (free!) and nowadays AI-based translations have been out there for ages to avoid language barriers. Web browsers typically include such features, so there's no excuse.
Press, press releases and unknowing journalists convert original sources such as published papers into headlines and clickbait articles. Almost always, details and the real facts are lost. Mind also that barely any study gives facts, they give percentages, correlations and potential conclusions. We already had an example above regarding red meat. Once you see "A study has found…", it's time to find the source and read it yourself. There are few good journalists in the health space (example: Gary Taubes who's much more a researcher than a hype texter), and in general, newspapers and other indirect summaries should be avoided. Nowadays, some researchers offer newsletters and podcasts that sometimes summarize articles and scientific literature. Those can be a good alternative to get a quick overview. Example: Harvard has published multiple headlines about red meat in the 2020's, often shamed by scientists. Please read more than just headlines and news articles. The science behind this is important, and here also what was considered (processed) red meat, how food intake was collected and evaluated, whether's it's observational data, and so on. Our previous family generations had no choice but to get the "latest" health information from newspapers sometimes. It's not a good alternative anymore (never has been).
"Extremist" bubbles: These are hard to define because many extreme opinions have some truth and reason. But not all! There are groups like missionary vegans, anti-vaccination, esoterism, carnivore dieters. Can you clearly judge them? Lots of snake oil, but also lots of potential benefits might be hidden in some of those ideas. Let's be explicit for once: in that mentioned list, it's reasonable to consider vaccine risk vs. benefit, and a carnivore or other exclusion diet (sometimes close to ketogenic diets) can be beneficial as well. The other mentioned items are snake oil or not health-related "extremism", not relevant for your research. Good health often lies somewhere in the middle. Science found many U-shaped correlations (example: carbohydrate intake vs. mortality, or LDL-C). However, in some health conditions, for example epilepsy, extreme solutions like special diets can be the solution, even if the general population doesn't need them. Again, one things can be both true and false. Avoid staying inside a box of thinking. Interest groups don't have the vigor to read all relevant information for a topic, but are usually limited, on purpose, to their world view. While points like animal protection and avoiding killing animals is a very fine goal in vegans, for instance, there are others to consider: is meat production better or worse for the environment (compared to vegetables, replacement products, etc.), are vegan diets healthy or unhealthy for certain illnesses or mortality in general, and so on. This article explicitly makes no judgement here. It's a complicated topic, and the author of this guide focuses on own health, while others might want more influence on world politics. Choose your bias, or better not. Let's also mention the term "cherry-picking" which means selectively choosing facts, studies, or arguments that support their views while ignoring contradictory evidence. The solution is the same as before: read everything, from all sides, prefer evidence, data and self-experimentation over opinions.
Trusting only one type of sources: If you only listen to people's anecdotes, the risk of drifting into a one-sided view is large, and thereby also actual health risks like side effects. As example, let's say you found many people reporting about ashwaganda online, and even in popular podcasts. You don't read public health warnings or scientific studies about the supplement risks. You get symptoms like brain fog and fail to make the connection for several weeks. Oops, that could have been prevented: you should know possible benefits and risks before trying something out.
Old studies: Science has come a long way in study design. While in the early 19th century, and definitely the centuries before, scientists were very vigorous in trying even the craziest experiments: cutting up the human body and finding what its organs do, staying in a cave to investigate how the body ensures the circadian rhythm, and countless more. Knowledge doesn't stay the same, though. Many countries of the world have small and large research institutions that bring all fields of health forward, including new and alternative theories. Always include the latest information in what you're reading.
Social media only: Reddit and other platforms can be a great source of information, as mentioned. But they must not be your only source. Forums and other platforms with post-and-comment functionality share a large problem: people are posting an extreme number of questions, and other people are posting lots of comments. Moderators often even remove content that remotely looks like medical advice or medical success stories. So the picture you get from looking only on Reddit is skewed at best. You can't only look at post titles like "XYZ helped me". Comments and other posts are important as well. As said above, you can neither trust upvotes nor the automatic comment ranking. The solution that your body needs might be deleted, downvoted into oblivion or hidden in one of the hundreds of similar questions and answers that you didn't read yet. Read a lot, and consider everything as both possibly correct and possibly incorrect. Here's an example: in the r/migraine subreddit, this post, one out many that hypes McDonalds fries and coke against migraine, is upvoted over 350 times until it got deleted by the original poster for unknown reasons, but has zero data or scientific backing, while another post, which explains effect and safety of salt supplementation based on real N=1 data, could not get any upvotes because it was deleted for forum rules ("No direct medical advice" allegedly applied). Given this often surprising kind of forum moderation which places solution and research posts at disadvantage, you may find a bad proportion of helpful posts despite being in a space that is supposed to help for a certain symptom or disease. Instead, you will find a larger proportion of questions and short comments from people who have not solved the issue yet. Even the time at which something got posted, given that people in the US are the major part of Reddit users, has a large impact on what gets upvoted and shown on users' home screens! Bias everywhere! Try a Google search query like site:reddit.com -inurl:?tl= migraine fixed to search specifically on one site (the "inurl" trick avoids translations to see the original language content), open several articles in browser tabs, then read through them. Check for references to studies, look them up on PubMed (sometimes the paywalled full text can be retrieved through your library's access system), check evidence, effects and risks for the findings.
Evidence-based science only: If you only rely on evidence-based science, you won't get full chances to find out new things. For example rare or new findings. "Functional medicine" is a somewhat new field in health, for instance. It has both snake oil sellers and very professional doctors and researchers. This field is more likely to help with rare conditions like MCAS by considering blood or other tests that aren't common in regular medical practices. Try to see which medical expertise, scientific information, anecdotal reports and own observations can help you. Everything might be helpful.
"Experiments have to be replicated": There are enough examples in scientific history where huge claims were made but then other labs, facilities or researchers could not reproduce the same results. Always get multiple sources and in case of scientific papers, at best a review with meta analysis, plus some anecdotes. Refer to the above "how to read a study" links to easily detect studies that are funded by the company whose product gets studied, meaning a high risk of bias towards producing a positive result or conclusion even if the data doesn't support it. Example: a marine oil product tested for effects on ADHD. Look at table 6 of the subjective, parent rating outcomes. You can see that the intervention and placebo groups both saw similar, strong improvements. This means that the subjective parent scale isn't very useful, which applies to other such studies as well, but the product also seems not more effective than placebo. The "Discussion" section of the study even says this: "The results of this study did not support the hypothesis that [name of product] would improve parent-rated levels of hyperactivity, inattention and impulsivity [...] over placebo." Also, the study didn't go that well: "low completion rate [...] There were 24 participant dropouts". Quite honest, right? No, because nevertheless, someone smuggled a positive rating into the "Abstract / Conclusions" section, even if the rest of the study says otherwise: "The results presented indicate that [name of product] may be beneficial in reducing levels of hyperactivity and inattention in a population of children with clinical and subclinical symptoms of ADHD." The study states that it was funded by the company that produces the product. This kind of fraud, deception or lobbyism happens all the time in science, so always remain aware of it!
"The top 10 things that helps your XYZ" articles: These articles flooded the internet even before AI-generated articles came around. Their quality is usually very bad and the authors mostly just copy from other sources. Better go and find original sources which don't claim (for example) that minor things help against a major disease. Unfortunately, this kind of resource pops up first in your Google search, so see if other search terms yield better results (e.g., "migraine dizziness treatment studies" instead of "migraine dizziness help").
Good information source, but bad content: this post is in the r/migraine forum, a reasonable place. The author claims to have reduced migraines from 15 per month to 2. However, the monthly numbers vary a lot, and the "2" in there is nowhere to be seen. In fact, the author posted on February 10th and included data for the incomplete February, mentioning 1 headache in that month. In a comment, there's someone who can "literally see the drop month over month", but the data doesn't show that at all. The only hint is potentially lower headache in Januar and less than half of February. Using the data that doesn't show anything (yet), the poster and commenters even make claims about magnesium and blue-light blocking glasses. With the post title "I managed to reduce the number of migraines", this is a typical incorrect and therefore unethical story to share. It's too late though – it got over 70 upvotes and people probably now focus on the claimed remedies for their own migraine instead of remaining open-minded. You may say that it's their fault for believing things that can't be seen in the data, but the damage isn't only on the people who upvoted! It's also in people who search for solutions in the future and stumble upon that post, or who use search and AI engines that are trained with such public data and likely repeat claims that appear many times on the internet, no matter how unfounded they are.
Scientific-sounding source, but backed by product monetization: check this ADHD expert ripping apart someone claiming that the disease can be improved with certain dietary choices. An unclear theory is presented very shortly, and "luckily", the original video author offers a paid cookbook. Mind: new theories of real pioneers can be a great resource, and "we would have found out a long time ago if this were true" isn't always a correct statement. New theories may lead us into directions that bring new research, solutions for subgroups or even larger groups of patients, or even find a biochemical explanation and cause for a disease. The likeliness that a video influencer, who also offers a paid product, has a great, working theory with large effect size in real patients – well, judge yourself, of course. It's great that "reply" videos like this one can sometimes be found, and if they're from an expert in the field, they can be a much greater resource, and less waste of time, than trying to make sense of the original video yourself.
Your own early or wrong assumptions: It's hard to catch own scientific mistakes. Check some example stories such as the one above, and see if you can catch yourself doing the same. Early assumptions are an obvious mistake – for example, thinking that some remedy helps within a few days against headache, when of course it needs months of data to prove that. Other mistakes are much more complex. Let's say you tried a few things against headache, and in the statistics, you find that 200 mg magnesium helps you, while 2x200 mg helps much more. If you have enough data – several months of trying either dosage and also days without magnesium – your logical conclusion is that the higher dose is better? Well, that's actually quite probable and if both dosages show much better results than taking zero, there's good reason to try the supplement further. Remember that these are contrived examples, not at all some praise of magnesium! But what if you tried or took something else in the same time frame, or tried a different diet, and magnesium is a full confounder, not having an effect on you at all? That can be excluded by writing down all interventions that you do, and either not doing them at once, or checking what happens on days where you did intervention A but not B, B but not A, or A and B combined. Another possibility: what if it's the time of magnesium intake, the second pill (of the "2x200 mg" dosing) being in the afternoon or evening, that has the effect?! In this example, it's actually probable because magnesium can have a calming effect. There can be a vast number of cofactors and variables. Even the symptom itself can be varying, such as headache being stronger on sports days, in summer, during weather changes, or having several independent triggers (which is common). There can also be "anti-cofactors": if I eat only meat for a week, and my health problems fully disappear, you can't immediately claim that meat is the solution, but rather you also need to consider what you didn't eat because of that diet, which may lead you to food items that were harmful for you all the time.
Document findings for yourself
The results you get from analyzing your data are most important for yourself. Having just a tool that shows some bar charts isn't really enough. You may want to take notes of what you found, and it's very individual how people do this. As author of staty, I write a journal of findings, and also maintain a correlation table (also as Google spreadsheet) where I enter ++/+/-/-- effects of input X on outcome Y (for example "Chocolate on sleep: ++"). The correlations can largely change over time, so I write down the date when I analyzed something, and add a link to the analysis as well. This way, I can easily trace back to what I did, and thereby later learn whether I made mistakes or misinterpreted something. You can save links of staty analyses as bookmarks to open them again later. That's also an easy way for not having to enter the same things into the analysis form every time.
Maybe some of the above ideas may work for you as well? Start a simple journal in a Google Doc or physical notebook, add a second sheet in your Google spreadsheet with correlations, a monthly calendar reminder to see if health outcomes have improved?
Share findings responsibly
We've learned above that online posts and comments by random strangers can be both very helpful, but also very unfounded with no proofs or data behind them. The effect on other people reading them can be strong. That's why N=1 scientists (like you?!) should be aware and tell their stories in a reasonable, fact-based, non-exaggerating way. Only once you have obvious, significant results (or negative results showing a non-effect!) over a longer time frame, it makes sense to share. That's because you can only judge safety, effectiveness and cofactors after a while. Here are a few tips:
- Don't generalize to other people. A finding or correlation in your data, no matter how strongly causal it looks, can be very different for others. Health issues can have a myriad of causes and influences and there's absolutely no way to remotely diagnose anyone without good inputs.
- Your conclusions and best solution of today could be retracted in a few months when you find a better explanation. An example: I found salt supplementation to be incredibly helpful to prevent my migraines. A very strong reduction in my headache frequency and strength proved that it worked for me. I planned a blog article already but wanted to observe the data a little longer. Some months later though, the relation to dizziness became apparent. So I added that as clear warning to the blog post. About two years later, I finally managed to consistently get into nutritional ketosis by diet, and that brought headaches to almost zero. It wasn't clear yet if the salt supplementation, which I had ditched for a while due to the dizziness risk, was still needed to keep up a reasonably low number of headache days. An update or new blog article for these observations and new questions would be great for interested people, but again needs to wait until enough data was collected with clear findings. Without the safety warning about dizziness, people may have tried the intervention without concerns after reading my blog post, probably resulting in problems that they don't understand could come from the additional salt.
- Most internet content doesn't come as detailed, data-backed blog post though, but as much shorter social media comments. So if you communicate your own story through online comments, please do take some care to put things into good words and explain all observations in certain detail.
Risks of self-experimentation
We already mentioned that supplements or medication can have strong side effects, and even lead to death. You've read the warning that a visit to your doctor or healthcare provider should be the first thing you do. Whatever you try on yourself, be it from informed sources such as this website or science papers, or other sources, like social media posts and videos, you take the full liability for your own health. Nothing on this website is professional medical advice. We focus on teaching science, allowing anyone to apply it to their own health, making reasonable decisions for or against health actions.
In particular, here are a few specific warnings, just to be sure we're on the same "path":
- Never replace or fully rule out conventional medical care. As for other areas, you don't want to get stuck in a dead end, excluding treatments that you're not even aware of yet. Try to learn about every area of medicine and see which can help you when and how. The purpose of this guide is definitely not to replace or speak ill of existing health systems, but to optimize your own health outcomes.
- Always be ready to stop experiments. While worsening of symptoms does not immediately equal that an experiment isn't working – time-limited "paradoxical effects" are possible – you must judge adverse events and observations to not risk your health. Some supplements and medication have such a strong effect on the body that they cannot even be stopped, and instead need to be carefully tapered off to avoid dangerous withdrawal effects. Think of people trying to stop cigarettes or alcohol, but worse. Be careful and check risks before any experimentation.
- Understand your health baseline. Which illnesses or health conditions do you already have? Could experiments interact with them in a bad way? Could you be pregnant or are you breastfeeding? Risks, intake recommendations and safety limits can differ a lot for certain conditions, ages, genders and population subgroups. And yes, this sound too much like we only mean pills here: sports, activities, lifestyle and diet changes… they can all have risks as well.
- Emergencies stay emergencies. They are not the time for experimentation. If something bad happens during an experiment, call an ambulance and make sure that you've updated your phone's emergency information in advance. Be honest with paramedics and doctors.
The end – you're an N=1 scientist now
Congratulations, you made it through this long guide 🏆! All the above takes practice and experience to be useful, but we were only able to explain some theory and examples in this article, not transfer scientific principles or decision-making experience into your brain. We wish you all the best in your health journey. Feel free to come back to this article to verify what you're doing.
After a while, maybe shortly watch the video "The epidemic of the "I Know All" expert" and check if you mistakenly became an "I Know All" expert instead of the critical, logically-moving hobby scientist that this article wanted you to learn to be. If we failed here, or you have any suggestions for this article or our guides, please send us feedback.